Long term regulation of Blood Pressure
- It helps in regulation of blood pressure over a prolonged period of time.
- Kidney plays an important role in long term regulation of blood pressure.
- It begins in few hours after change in Blood Pressure and continues for days to weeks.
- The long term BP regulation is mainly done by regulation of extracellular fluid volume.
Three mechanisms are involved in the long term regulation of
Blood Pressure
- Renin-Angiotension-Aldosterone System (RAAS)
- Tubuloglomerulo feedback
- Thirst mechanism
1) Renin-Angiotension-Aldosterone System (RAAS)
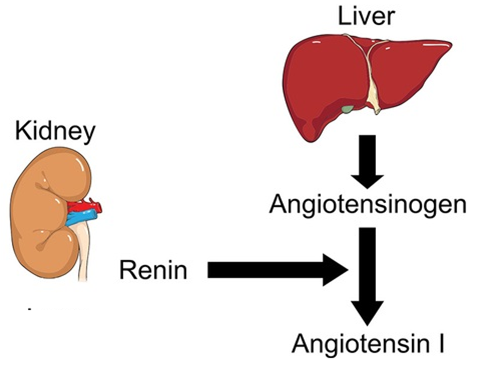
- The Juxtaglomerular apparatus senses decrease in the blood pressure and secrete a hormone called Renin.

- Renin catalyzes the conversion of Angiotensinogen (produced in liver) to Angiotensin I.
- Angiotensin I is converted into Angiotensin II by the action of Angiotensin Converting Enzyme (ACE) present in the endothelium of blood vessels in the lungs.

- Angiotensin II has three effects by which it increases the Blood Pressure
b) Decrease in salt and water excretion by kidney
c) Stimulation of thirst
a) Vasoconstriction
Angiotensin II being a potent vasoconstrictor, cause
generalised vasoconstriction of arterioles and veins there by increasing both
systolic and diastolic Blood Pressure.

b) Decrease in salt and water excretion by kidney
ii) Indirect action on the kidney
i) Direct action on the kidney
- Angiotensin II constricts the efferent arterioles which diminishes blood flow through the peritubular capillaries, allowing rapid osmotic reabsorption from the tubules.
- Angiotensin II directly stimulates the epithelial cells of renal tubules to increase reabsorption of sodium and water.
ii) Indirect action on the kidney
- By stimulating secretion of Aldosterone.
- Angiotensin II stimulates the Adrenal Glands to secrete Aldosterone which in turn increases salt and water reabsorption by the epithelial cells of the renal tubules.

c) Stimulation of thirst
- Angiotensin II is a powerful stimulator of thirst.
- It leads to consumption of large volumes of water, leading to a rise in blood volume.
2) Tubuloglomerulo feedback
- Angiotensin also cause release of Anti-Diuretic hormone from Posterior pituitary.
- ADH increases water reabsorption there by increasing the body fluid volume and Blood Pressure.

3) Thirst mechanism
- By initiating thirst mechanism there is increase in extracellular fluid volume > increase in blood volume > increase in Blood Pressure.

Blood Pressure: Applied Aspects
- Blood pressure is usually maintained with in a narrow limit in a healthy individual
- It can increase or decrease above the normal limits in pathological conditions
- Increase in blood pressure above the normal limit (120/80 mmHg) is known as Hypertension
- Decrease in blood pressure below the normal limit (120/80 mmHg) is known as Hypotension
- Both Hyper and Hypo tension is dangerous for life.
Hypertension
- Condition in which blood pressure is persistently above 140/90 mmHg
Major cause
- Atherosclerosis

Complications of Hypertension
- Cerebral haemorrhage
- Thrombosis in cerebral blood vessels
- Stroke
- Heart failure
- Renal failure


Primary hypertension
- Also called Essential hypertension.
- 90% of patients – cause unknown.
- May be due to neurovascular compression of rostral ventro-lateral medulla.
- Effective lowering of blood pressure can be achieved by use of conventional anti-hypertensives.
Secondary hypertension
Secondary to a disease affecting the other systems
- Renal hypertension
- Coarctation of thoracic aorta
- Pill hypertension
- Pheochromocytoma
- 11β-hydroxylase deficiency
- Cushing’s syndrome
Malignant hypertension
Long standing hypertension – shows necrotic arteriolar
lesion
Condition associated with
- Papilledema
- Cerebral manifestations
- Renal failure
Can be reversed by suitable antihypertensive therapy

Management of hypertension
Why required?
Persistent increase in blood pressure
▼
Damage to internal organs
▼
Greater risk of cerebrovascular accidents
Hypertension is managed by
- Pharmacological methods
- Nonpharmacological methods
Pharmacological methods of management of Hypertension
By usage of various drugs
- Diuretics
- β-adrenergic receptor antagonists
- Calcium channel blockers
- ACE inhibitors
- Angiotensin II receptor blockers
- Vasodilators
Diuretics
Reduce fluid volume
▼
Reduce venous return and cardiac output
▼
Reduces blood pressure
Eg: Furosemide, Amiloride

β-adrenergic receptor antagonists
Blocks β-adrenergic receptors present in cardiac muscles
▼
Reduces myocardial contractility
▼
Reduced cardiac output
▼
Reduces blood pressure
Eg: Propranolol

Calcium channel blockers
Reduce the availability of calcium ions to myocardial cells
▼
Reduces myocardial contractility
▼
Reduced cardiac output
▼
Reduce blood pressure
Eg: Amlodipine

ACE inhibitors
Prevents conversion of Antiogensin I to Angiotensin II
▼
Blockage of vasoconstrictor effect of Angiogentsin II
▼
Reduces blood pressure
Eg: Captopril

Angiotensin II receptor blockers
Blocks Angiotensin II to bind to its receptors
▼
Blocks vasoconstrictor effect
▼
Reduces blood pressure
Eg: Losartan

Vasodilators
Act directly on the smooth muscles of blood vessels
▼
Vasodilation
▼
Reduce peripheral resistance
▼
Reduce blood pressure
Eg: Sodium Nitropruside

Nonpharmacological methods of management of Hypertension
- Diet
- Modification of risk factors
- Relaxation and exercise
Diet
- Correction of obesity by regulating food intake
- Reduced consumption of alcohol
- Decrease salt intake
Modification of risk factors
- Reduce smoking
- Effective treatment of hyperlipidemia
Relaxation and exercise
- Relaxation and regular exercise can lower the blood pressure by improving physical fitness and reaction to stressful stimulus.
Non pharmacological management can by used as an adjuvant
for pharmacological management
Hypertensive Myocardial Hypertrophy
Hypertension
▼
Increased after load to left ventricle
▼
Left ventricle generates greater force to eject blood
▼
Prolonged increase in after load increase contractility
▼
Increases the thickness of ventricular wall
▼
↓Capacity of lumen and compliance of myocaridum
▼
Diastolic failure

Hypotension
Decrease in BP below the normal value of 90/60 mm Hg
Eg: Circulatory shock
Effect of posture on blood pressure
change in posture : lying to standing

- This will stimulate the Baro-receptor mediated compensatory response to restore blood pressure.
- Venous pooling in lower limbs can cause fainting spells when the posture is suddenly changed from lying to standing.
- Edema in lower limbs after prolonged standing is due to an increase in capillary pressure on account of gravitational force and filtration of fluid into the interstitial space.
Valsalva maneuver
- Exhaling against a closed glottis
- Tests the integrity of the Baro-receptors

Mechanism of Valsalva maneuver
Exhaling against closed glottis
▼
Increases intrathorasic pressure
▼
Decreases venous return
▼
Reduces cardiac output
▼
Reduces blood
pressure and blood flow to
Baro-receptors
If Baro-receptor reflex intact
▼
Sympathetic discharges to heart and blood vessels increase
▼
Increase in heart rate
On stopping the maneuver
▼
Venous return increases
▼
Increased discharge from baro-receptors
▼
Reduces the heart rate
Hypertension
- Rupture blood vessel

Hypotension
- Reduced tissue perfusion
